Loading...
Payment solutions for all businesses
Grow your revenue with payment solutions designed for the entire customer lifecycle.






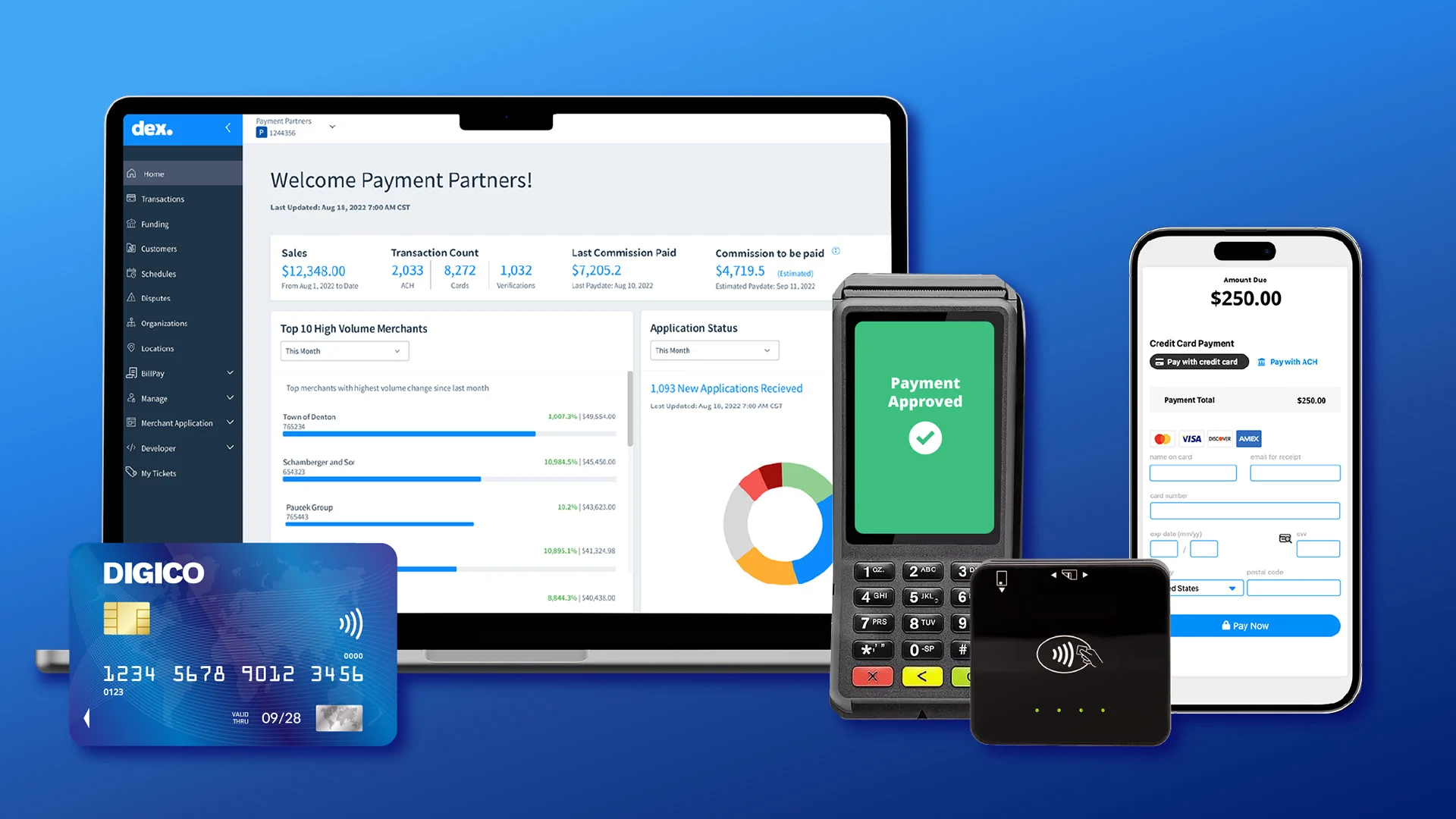
Unified Payments Platform
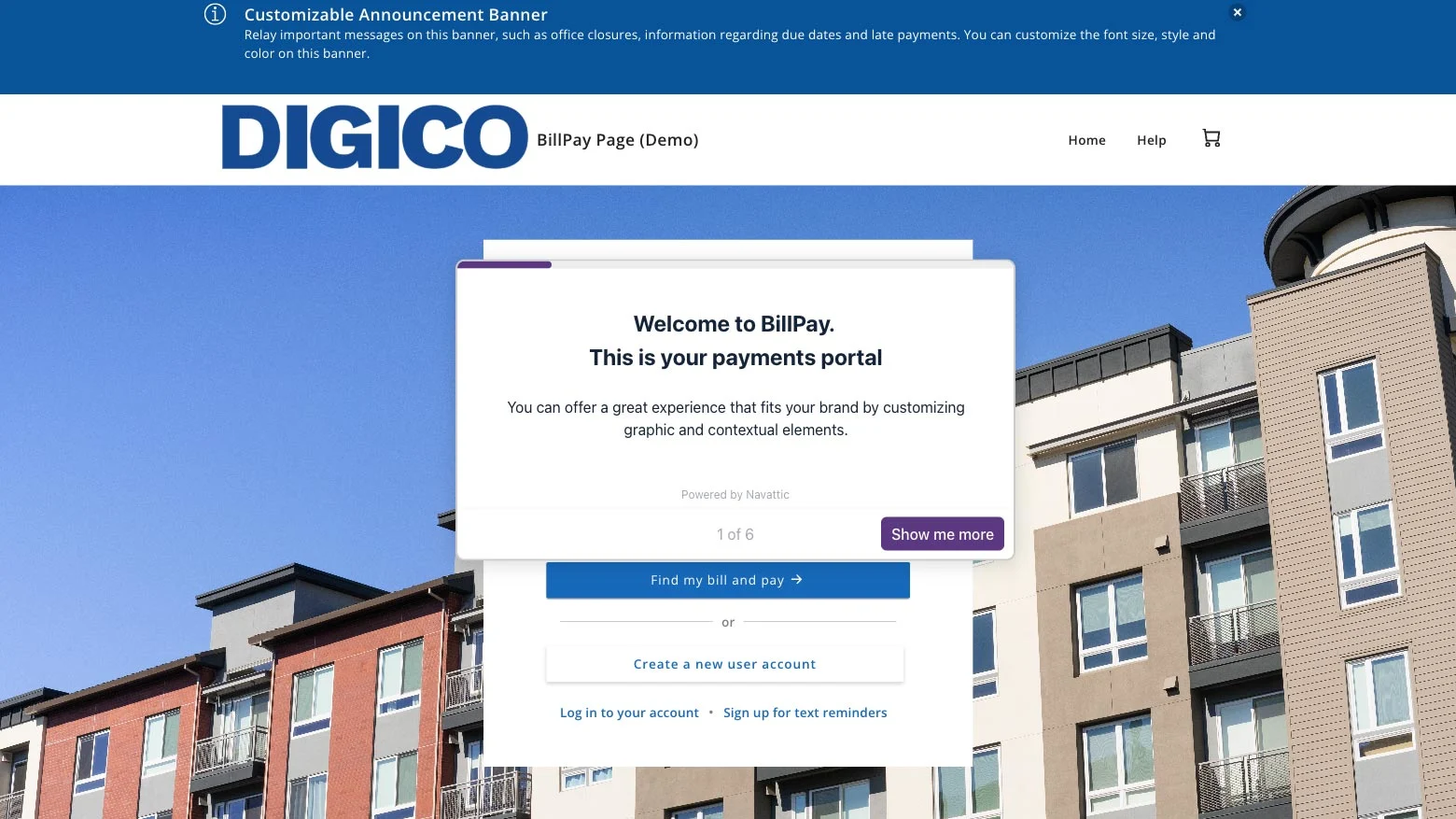
Allow your customers to pay how and where they want
Continue to evolve as your customer’s buying behaviors do by providing payment options that fit their lifestyles and grow your business (or revenues).
Enterprise-grade stability to manage billions of billing, payments and customer engagements each year

260M
transactions processed annually
25+
years of experience
$195B+
in annual payments
175K
worldwide merchants
Market fluency
Purpose-built for your industry
See why businesses rely on CSG Payments to power their full potential.
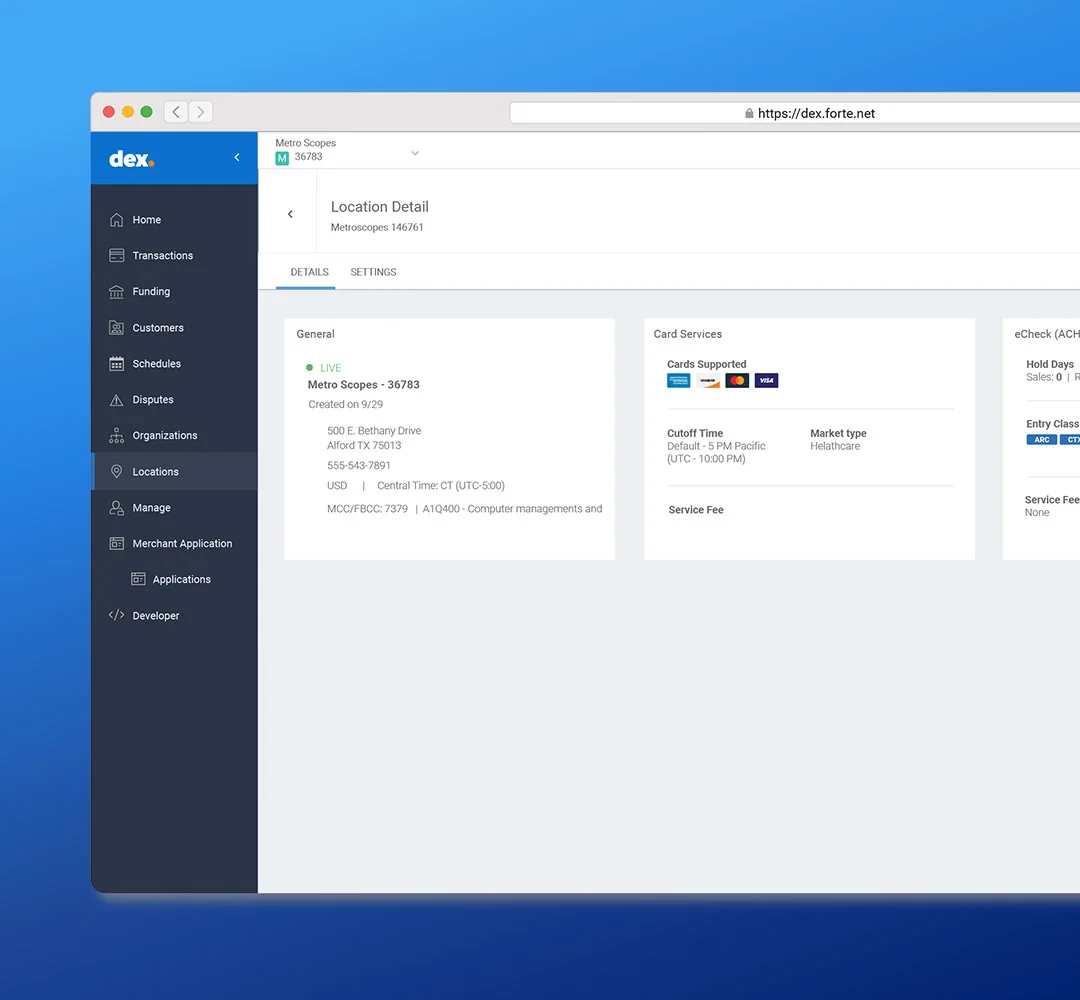
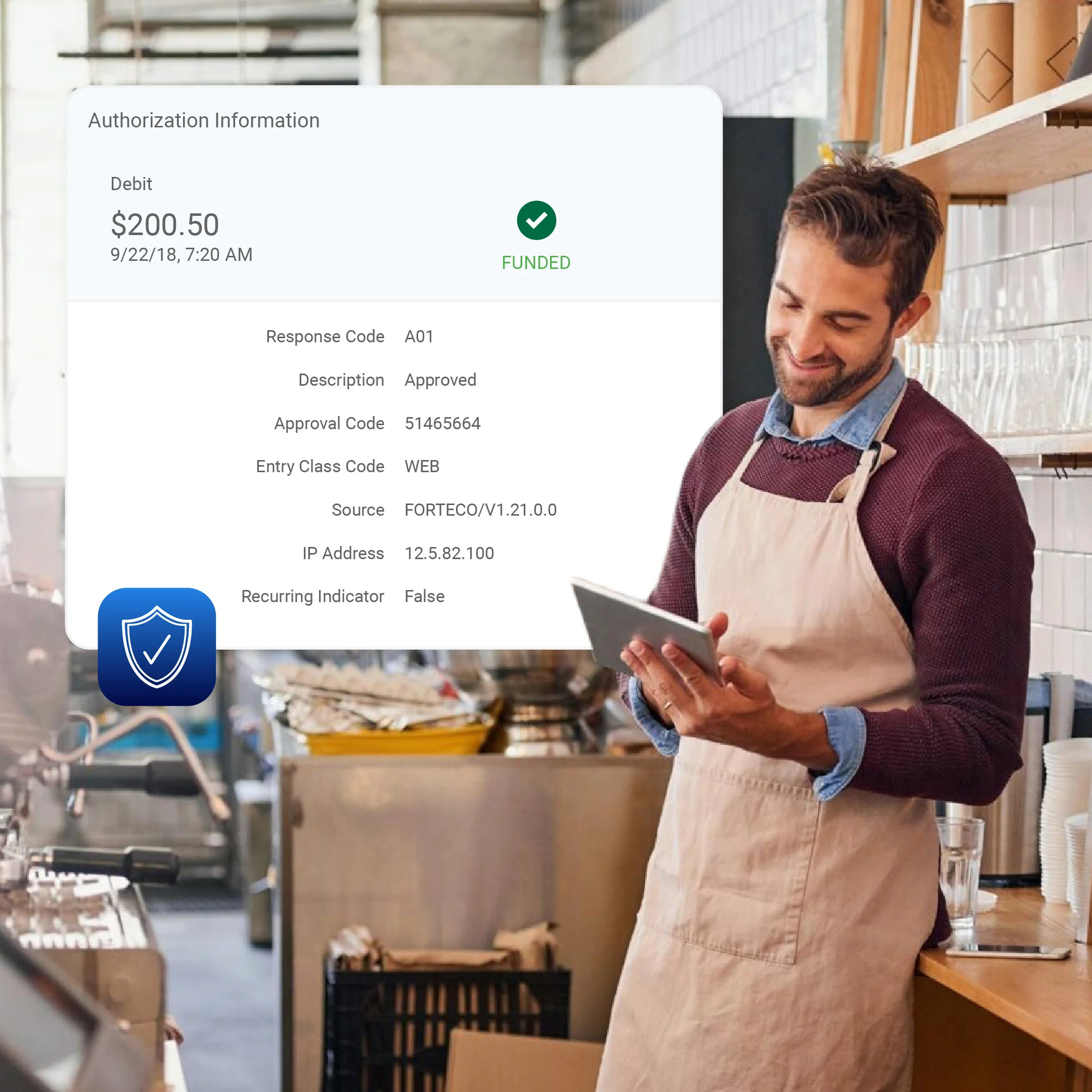
Focus on patient care, not payment paperwork
Streamline payment collections with HIPAA-compliant payment options. Whether you’re taking patient payments or closing insurance claims, we remove the manual work so your providers and facilities get paid faster.
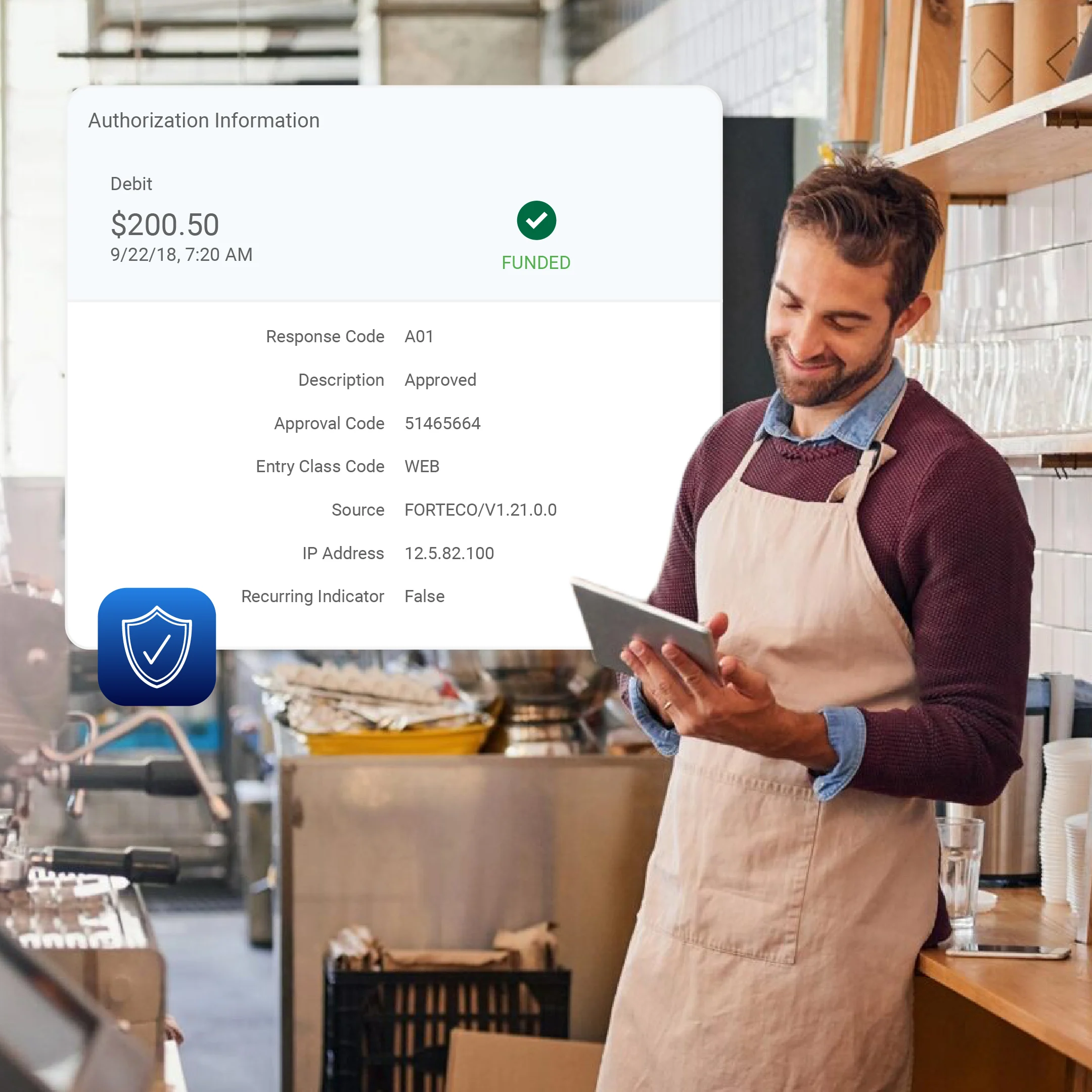
Make payments your competitive advantage
Start taking payments almost immediately with our self-service onboarding. Give your customers the modern, fast experience they expect. Save money on every transaction with cost-effective ACH/eCheck processing, ideal for recurring billing models.
Customer Stories
Where market leaders go to grow
When industry leaders need to move billions of dollars without error, they rely on our infrastructure.

From a flow standpoint, from the client side, it just feels easy and like how it’s supposed to be.
Thomas CarconeCo‑founder/Co‑owner
Thomas Carcone Co‑founder/Co‑owner
One thing you don’t want to do as a merchant is worry about your processor; with NCMS and CSG Payments, you don’t have to.
Scott Lewis President & CEO
Scott Lewis President & CEO
I absolutely love CSG Payments. It is just the greatest thing ever.
Rosie AlfaroDimmit County Court Clerk
Rosie Alfaro Dimmit County Court Clerk
CSG Payments' ability to handle service fees and online bill pay made a significant difference. This was a huge win for us and our customers using WasteWORKS
James BlantonChief Financial OfficerWasteWORKS
James Blanton Chief Financial Officer WasteWORKSCSG Forte for Payments
Expert analysis
Explore our latest thinking
Strategic insights and forward-looking trends to help you stay ahead of shifting customer expectations.



Security
Compliance that scales with your business
When you work with us, you’re working with a fully audited, secure, and compliant partner. From PCI compliance to broader data privacy, we safeguard your payments and sensitive information wherever you do business.

Grow your payments revenue with a proven partner
See our platform in action or discuss your integration needs with a specialist.